
A Clear Path to Sustainable Crisis Care
Paul Galdys, MBA, CPRP
Executive Principal Consultant

One-Time Funding Does Not Typically Result in Sustainability
States, counties, local municipalities, and communities throughout the nation have worked to improve access to specialized behavioral health crisis care for those in need. Efforts have been fueled by one-time funding opportunities through the federal government and financial commitments, such as levies, from local taxpayers; representing a significant financial commitment to stand up care that often lacks the financial structures needed to support ongoing mobile crisis outreach and facility-based crisis care. Sadly, some of these newly created programs have already closed and many more are at risk.
The last five years have seen a dramatic increase in efforts to advance crisis care. Spurred by:
SAMHSA’s 2020 release of the National Guidelines for Behavioral Health Crisis Care;
Increased prevalence of individuals in acute behavioral health distress during the 2020 COVID pandemic;
The 2022 designation of 988 as the nation’s suicide and crisis lifeline; and
The 2025 release of SAMHSA National Guidance documents,
Communities throughout the country have worked to offer immediate access to care for those experiencing an emergent behavioral health crisis. Enhanced SAMHSA, COVID Relief, block grant set-aside allocations for crisis care, and American Rescue Plan funding has fueled efforts to offer (1) someone to contact (crisis lines), (2) someone to come to you (mobile crisis outreach), and (3) safe places for help (intensive in-home supports and facility-based crisis care) throughout the country. These one-time funding sources offered a path to stand-up care but were never intended to serve as ongoing dollars to sustain those critical emergency behavioral health services. Far too often, crisis care services are funded solely through state, local, and/or grant sources; creating a significant financial burden to local taxpayers to cover the cost of healthcare despite being predominately delivered to individuals who have healthcare insurance. For many communities, this will prove unsustainable and access to these vital services will be lost unless action is taken.
Tangible, Replicable, and Well-Established Solutions Exist
The first step is to acknowledge that behavioral health is a part of overall health and that behavioral health services (mental health and substance use treatment) are an essential part of a healthcare service continuum. The good news is that federal parity law establishes an expectation that this is true within healthcare law. Once one has embraced the premise that behavioral health services are essential part of a healthcare system, specific actions are needed to incorporate targeted services into that system. Those actions are needed to put these behavioral health services on par with their physical health counterparts in which a vast majority of the cost of an emergency medical service (EMS) response in the community or a visit to a hospital emergency department are paid for by the individual’s health insurance provider instead of local taxpayers. Let’s explore how to make this a reality.
The most promising path to crisis care sustainability is to integrate these services within the overall healthcare system. Integration within the healthcare system results in an approach in which insurers cover these services like their physical health counterparts (i.e., EMS and mobile crisis or hospital EDs and crisis facilities). Reimbursement strategies could incorporate fee-for-service, value-based, and prospective payment systems with rates that align with the cost of offering 24/7/365 access to the targeted crisis services. The steps to execute on this vision are relatively straightforward and essential to meeting federal parity law requirements that have been in place for years. Put simply, federal healthcare parity laws require that mental health and substance use disorder benefits be treated no less favorably than medical/surgical benefits in insurance plans.
State and Local Budget Impact
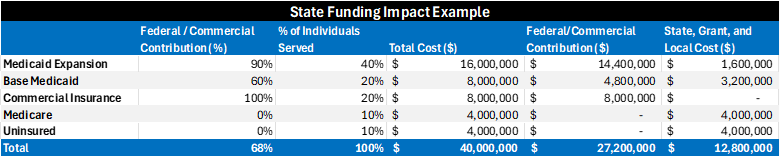
Let us explore the potential impact a few simple steps will have on a state budget that is currently funding crisis care through general funds and local levies. Let’s assume that this state operates mobile crisis outreach and facility-based crisis care at an annual cost of $40 million. Base Medicaid FMAP (federal contribution) is 60% in this state and Medicaid expansion is in place (which comes with a 90% federal contribution). For this scenario, we will assume the following insurance coverage for individuals who receive crisis care: 40% Medicaid expansion, 20% base Medicaid, 20% commercially insured, 10% Medicare, and 10% uninsured. The table (below) shows how leveraging Medicaid’s federal funding contribution and commercial insurers paying for the care of their members reduces the state and local spend from $40 million to $12.8 million annually which is a 68% reduction.
Step by Step
This section contains the steps needed to realize a reduction in state, local, and/or grant funding spend that supports to delivery of behavioral health crisis care services. These tangible, replicable, and well-established steps can help any state, including those that have not expanded Medicaid, shift to a more sustainable crisis care system by dramatically lowering the financial burden facing local taxpayers who are largely paying for healthcare services that are, according to parity law, the financial responsibility of their health insurer.
Step 1 – Incorporate targeted crisis services into your state’s Medicaid covered services. Many states have already done this so there is replicable publicly published waiver and state plan amendment language available to your state if needed. This should help states avoid further delay incorporating behavioral health crisis care services within the state’s Medicaid coverage in a manner that aligns with existing federal parity law.
Step 2 – Solidify fee-for-service rates for each of the targeted crisis care services. Please note that these first two steps are important even if primary Medicaid reimbursement for crisis care is through a PPS rate paid to CCBHCs because other payers with parity expectations will benefit from a service-specific rate established within the state. If rates fall short, sustainability will likely require taxpayer subsidy for each service delivered to Medicaid or commercially insured individual which will significantly increase state, county or local costs. Although commercial insurers should not establish parity compliance with reimbursement rates simply by relying on the Medicaid Fee Schedule, this often serves as an initial reference point in a state.
Step 3 – When appropriate, ensure emergency and urgent behavioral health services are designated as such within the state’s Medicaid program to solidify parity expectations. If managed care health plans are reimbursing for emergency medical and surgical services, then they must reimburse for their analogous emergency behavioral health services such as mobile crisis outreach and facility-based crisis care.
Step 4 – Partner with the state’s Department of Insurance or other designated branch of government responsible for enforcement of parity to secure commercial insurance reimbursement for targeted crisis care services.
Step 5 – Evaluate system design structure opportunities to incorporate an entity or entities responsible for working with providers to ensure appropriate levels of access are available. A strong system design can also identify ways of braiding funding to support care delivered to uninsured and underinsured (even Medicare) individuals.
Step 6 – Incorporate contractual expectations that crisis service providers bill all applicable insurers for services delivered to enrolled members.
Understanding Parity Law
The Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act of 2008 (MHPAEA), commonly referred to as the federal parity law, requires that health insurance plans offering mental health and substance use disorder benefits must provide coverage that is comparable to medical and surgical benefits. This includes emergency services for behavioral health.
Under MHPAEA:
Coverage limitations (g., copayments, deductibles, prior authorization requirements) cannot be more restrictive for behavioral health services than for medical/surgical services.
This applies to group health plans and insurers, including those serving Medicaid enrollees through managed care organizations (MCOs).
States and MCOs are required to conduct parity analyses to demonstrate compliance, and the Centers for Medicare & Medicaid Services (CMS) audits these analyses.
Additionally, the Affordable Care Act (ACA) expanded these protections by:
Mandating that mental health and substance use disorder services be included as Essential Health Benefits (EHBs).
Requiring that individual and small group market plans cover these services at parity with medical and surgical benefits.
Ensuring that emergency behavioral health services are covered without prior authorization and with the same cost-sharing as other emergency services.
Take Action Today
A tangible path to dramatically reduce reliance on local funding by treating crisis care as part of the healthcare system exists and can the steps discussed earlier offer a clear path to increased system sustainability. The physical healthcare system already applies this approach to EMS response in the community (analogous to mobile crisis outreach) and hospital emergency department care (analogous to facility-based crisis care). It should be noted that the impact table used in this discussion does not include any federal funding contributions for Medicare enrolled individuals, However, contracting with Medicare Advantage Plans is possible and, minimally, providers can bill Medicare for professional services delivered by licensed individuals as part of crisis service delivery. Each payment received through Medicare further reduces state, county, grant, and/or local costs for these vital services.
The steps to crisis care sustainability are replicable, align with parity law expectations, and will solidify systems that can offer access to care when someone is experiencing mental health and substance use distress in any community in the nation.
Resources
Parity Action Plan for Emergency Behavioral Health Crisis Care
Sustainable Funding for Mental Health Crisis Services
Office of the Assistant Secretary for Planning and Evaluation – Affordable Care Act Expands Mental Health and Substance Use Disorder Benefits and Federal Parity Protections for 62 Million Americans | ASPE
About the Author
Paul Galdys has more than 35 years of experience in the mental health, intellectual/ developmental disabilities, and substance use treatment field. Currently an Executive Principal Consultant with Recovery Innovations and a member of CIT International’s Board of Directors, past work includes overseeing crisis care operations in 10 states, Assistant Director with the Arizona Department of Health Services as well as Assistant Director in Arizona Medicaid. He’s a cited contributor to SAMHSA’s 2020 National Guidelines for Behavioral Health Crisis Care – A Best Practice Toolkit, National Guidelines for a Coordinated System of Crisis Care and Model Definitions for Behavioral Health Emergency, Crisis, and Crisis-Related Services.
Ready to Move from Planning to Action?